A Clinical Framework for DID Relationships
The Beach Safety Hierarchy
Five levels of nervous system readiness for relational engagement in Dissociative Identity Disorder and complex trauma — a validated model for partners and clinicians.
Polyvagal Theory · Attachment Theory · Sensorimotor · Window of Tolerance
Open Access Preprint doi.org/10.5281/zenodo.19688087The Problem
Intimate partners of individuals with DID, PTSD, and complex PTSD face a clinical challenge the field has named but not solved: how to calibrate relational behavior to a nervous system whose capacity for engagement shifts in real time.
Existing partner psychoeducation tells partners what to be — patient, consistent, educated. It does not tell them what to do when. Polyvagal Theory describes what the nervous system does. Attachment Theory describes what the system needs. Neither tells the partner what to do at 11 p.m. when a conversation collapses and no clinician is in the room.
The Beach Safety Hierarchy provides that structure.
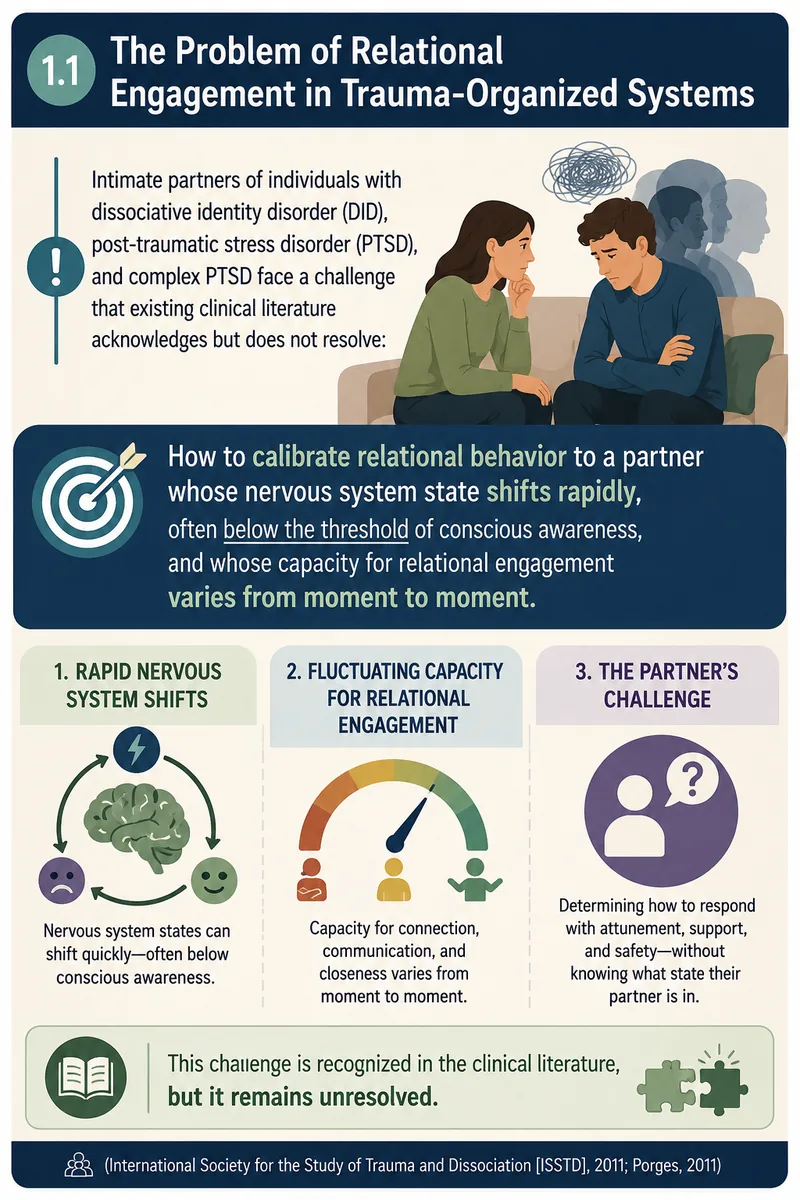
Figure 1.1 — The clinical gap the BSHAS is designed to address.
Theoretical Foundation
The Beach Safety Hierarchy synthesizes three established bodies of research that each describe a different dimension of the problem — but none of which, individually, provides a partner-facing assessment structure.
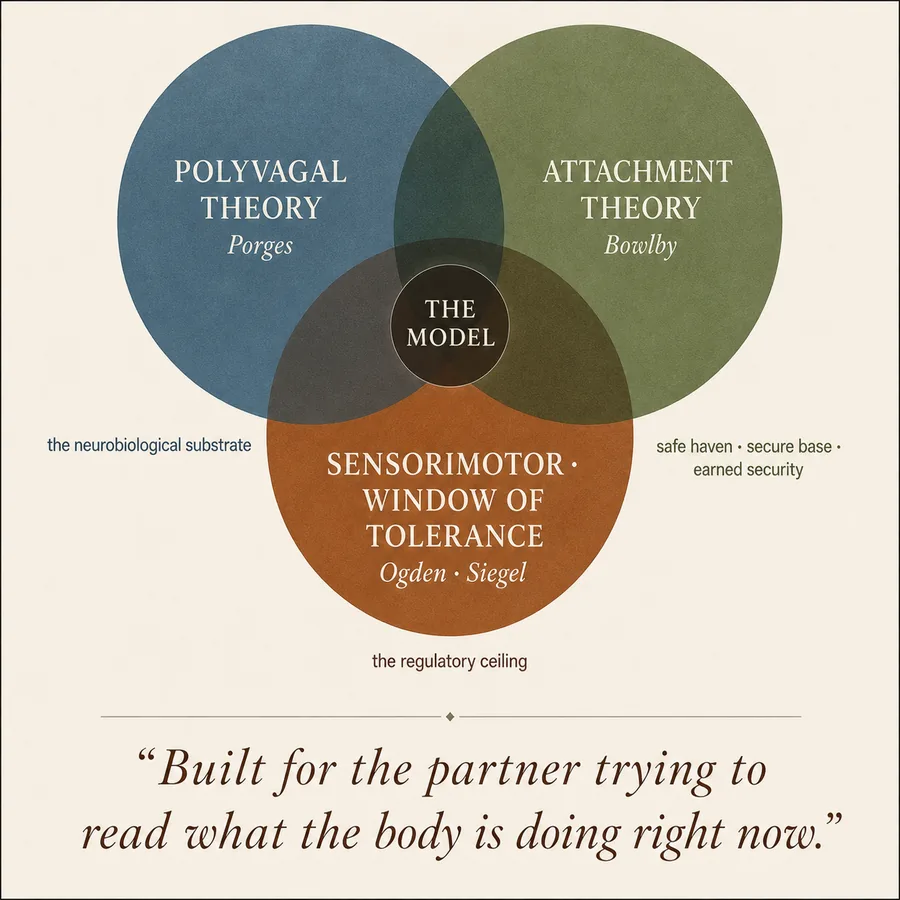
“Built for the partner trying to read what the body is doing right now.”
Porges’ (2011) Polyvagal Theory provides the neurobiological substrate: the autonomic nervous system evaluates safety through neuroception and gates access to the social engagement system. Bowlby’s Attachment Theory establishes the conditions for safe haven and secure base functioning. Siegel’s (2012) Window of Tolerance and Ogden’s Sensorimotor framework provide the regulatory ceiling: the zone of arousal within which integrative cortical processing is possible. The BSHAS operationalizes all three into a single hierarchical assessment structure.
The Five Levels
Nervous system readiness for relational engagement operates across five sequential, hierarchically organized levels. Three core principles govern the model: sequentiality (levels cannot be skipped), bidirectionality (the partner’s own regulation determines the ceiling of safety they can provide), and non-linearity (level position is dynamic and state-dependent, not a trajectory of improvement).
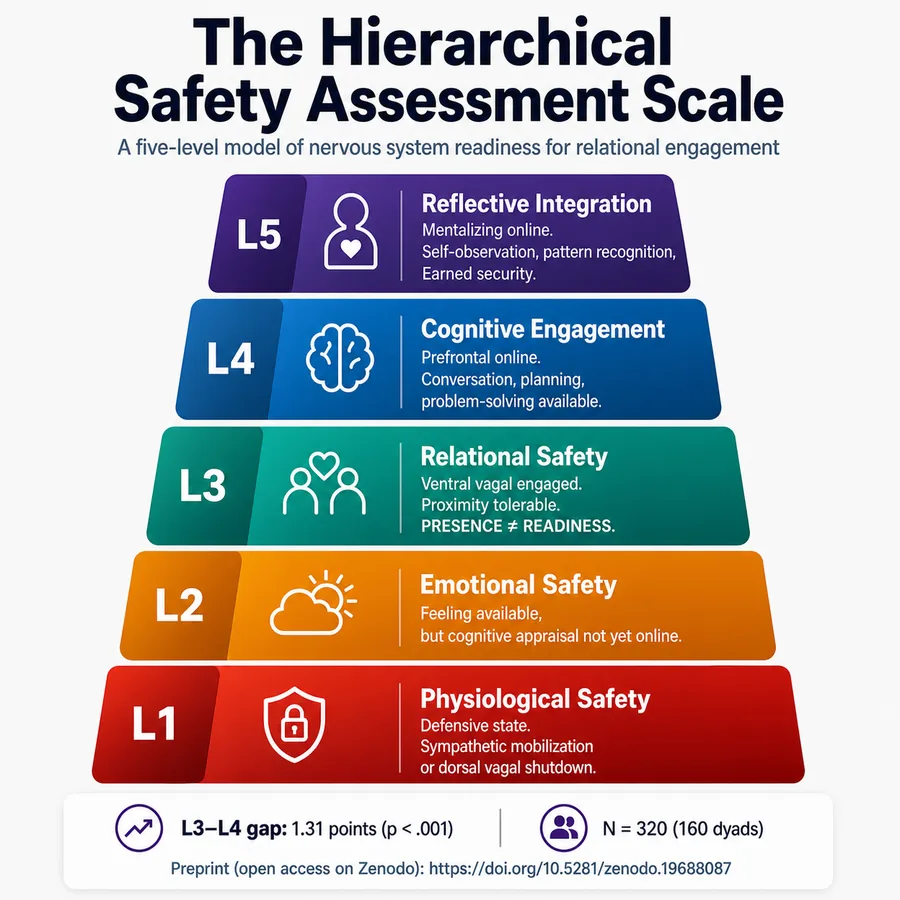
Level 1 · Physiological Safety
Core question: Is the body calm enough to be present in shared space?
The nervous system is in defensive mode — sympathetic mobilization or dorsal vagal immobilization. The social engagement system is offline. Verbal reassurance, logic, and emotional appeals are largely unavailable as regulatory tools at this level.
Level 2 · Emotional Safety
Core question: Can emotion be expressed without expectation of punishment, dismissal, or escalation?
The social engagement system is fragile but emerging. Emotional expression is available; cognitive appraisal, perspective-taking, and narrative coherence are not. The person can feel but cannot yet think about what they feel.
Level 3 · Relational Safety
Core question: Can the person be in relational proximity without defensive activation?
Ventral vagal engagement supports proximity and relational bids. This is the lowest level at which relational interventions function. Complex relational content, problem-solving, and planning are not yet available. This level is frequently misread as Level 4.
Level 4 · Cognitive Engagement
Core question: Can the person process relational content and participate in shared decision-making?
Prefrontal cortical processing is online. Conversation about the relationship, planning, problem-solving, and meaning-making are available. Deep reflective capacity regarding one’s own patterns is not.
Level 5 · Reflective Integration
Core question: Can the person observe their own patterns and revise their internal working model of the relationship?
Mentalizing capacity is online. The person can connect past to present, name their own defensive behaviors with curiosity, and hold two contradictory things as simultaneously true. Corresponds to the construction of earned security — and carries a collapse risk unique to this level.
The Key Finding
The most robust and clinically significant distinction in the data was between Level 3 (Relational Safety) and Level 4 (Cognitive Engagement) — a gap that is invisible to most partners and responsible for the most damaging relational misfires in trauma-affected couples.
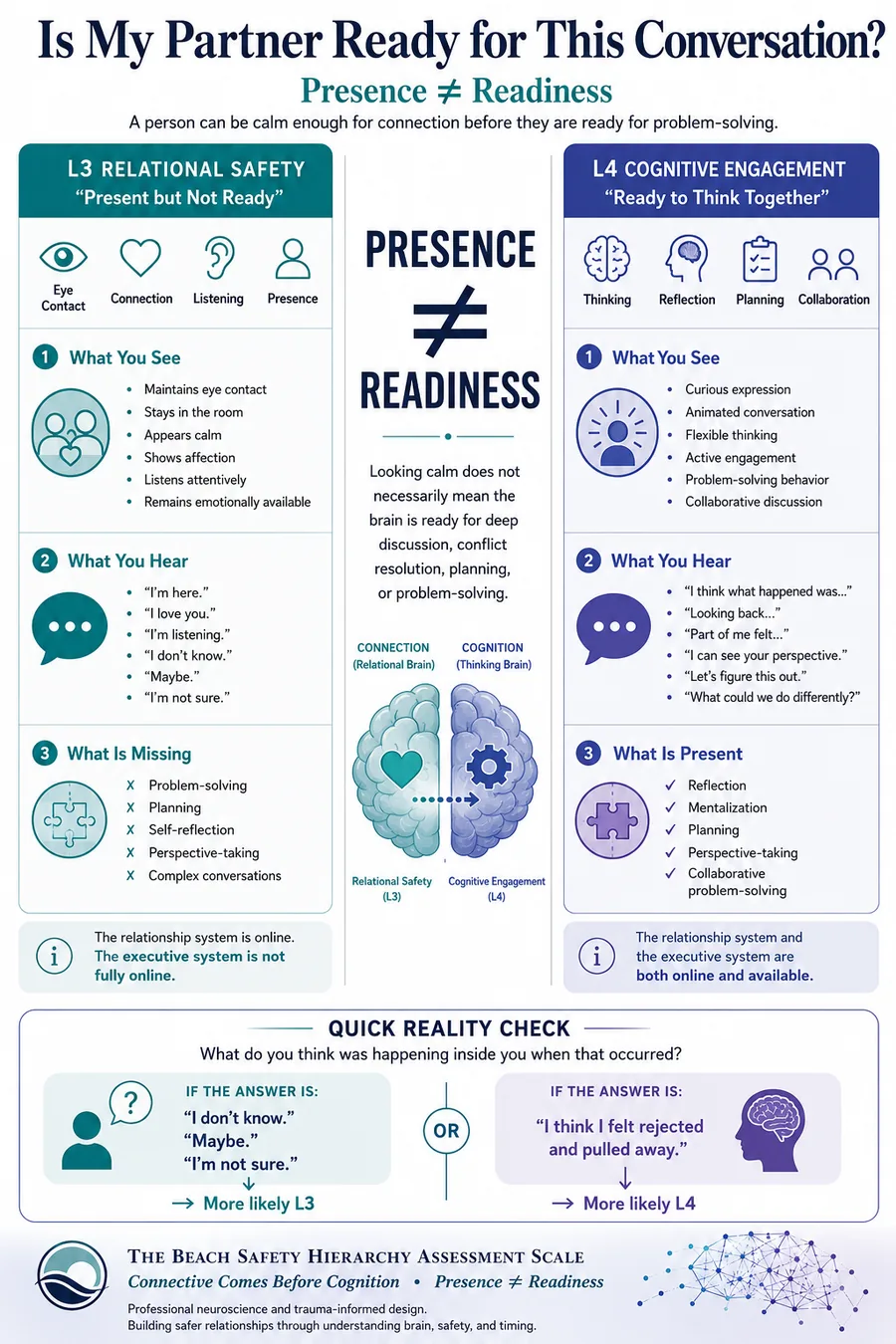
Figure 4 — The L3/L4 distinction: behavioral markers and the Quick Reality Check.
Preliminary validation on 160 dyadic pairs (N = 320) supports the hierarchical structure across both self-report and partner-report forms.
“Among respondents with relational safety online,
cognitive engagement dropped by 1.31 points on a 5-point scale
(p < .001).”
The moment the partner looks most ready for a hard conversation is measurably a moment when the cognitive processing to hold that conversation is often not yet available.
Within-pair concordance between self-report and partner-report ranged from r = .73–.85 across all five levels. Internal reliability: all subscales α > .80.
Clinical Grounding
The BSHAS draws on established peer-reviewed bodies of research. Each theoretical pillar addresses a different dimension of the relational challenge facing partners of individuals with DID and complex trauma.
Polyvagal Theory
Porges (2011) provides the neurobiological substrate: the autonomic nervous system evaluates safety through neuroception and gates access to the social engagement system. The five-level hierarchy maps directly to the polyvagal ladder.
Attachment & Mentalization
Bowlby (1982) and Fonagy et al. (2002) establish the conditions for safe haven and secure base, and define the pathway to earned security through mentalization — the capacity to observe one’s own internal states. Level 5 corresponds to active mentalizing.
Window of Tolerance
Siegel (2012) and Ogden et al. (2006) define the zone of arousal within which integrative cortical processing is possible. Levels 4 and 5 of the BSHAS require that both partners are operating within this window.
External Clinical and Academic Resources
- International Society for the Study of Trauma and Dissociation (ISSTD) — Primary professional body for DID treatment standards and research
- What Is DID? — Clinical overview on this site
- DSM-5-TR 300.14 — Diagnostic criteria for Dissociative Identity Disorder
- van der Hart, O., Nijenhuis, E.R.S., & Steele, K. (2006). The Haunted Self: Structural Dissociation and the Treatment of Chronic Traumatization. W.W. Norton.
- van der Kolk, B. (2014). The Body Keeps the Score. Viking.
- Porges, S.W. (2011). The Polyvagal Theory. W.W. Norton.
- Ogden, P., Minton, K., & Pain, C. (2006). Trauma and the Body. W.W. Norton.
Research Program
The BSHAS is a 25-item self- and partner-report instrument developed to operationalize the five-level model. The preprint, assessment instrument, and clinical applications are available through the links below.
Preprint
Full manuscript: development, factor structure, and preliminary validation. Open access, CC BY 4.0.
Download Free →Zenodo · CERN Data Centre
doi.org/10.5281/zenodo.19688087
Assessment Instrument
The 25-item BSHAS with parallel self-report and partner-report forms. Available for non-commercial research and clinical use.
For Clinicians
Partner psychoeducation, couples therapy with trauma-affected clients, phase-oriented treatment planning, pre-session readiness assessment.
Research Collaboration
Seeking co-investigators for longitudinal validation, intervention development, and clinical-sample replication studies.
The Book
Lead with Safety
A Husband’s Guide to Loving a Wife with DID
Visit the Hub →The clinical framework documented on this site provides the backbone of Lead with Safety, a narrative nonfiction book for the non-clinical partner of a person with Dissociative Identity Disorder or complex trauma. The book translates the five-level model into lived experience — what the levels look like at the kitchen table, at 11 p.m., in the middle of a conversation that just collapsed.
The BSHAS is the research instrument. The book is what it feels like to actually live inside it.
Articles, framework explainers, and partner resources at the companion hub: leadwithsafety.com
About the Author
Scott Beach is a Licensed Chemical Dependency Counselor (LCDC-II), Registered Pharmacist (RPh), and independent researcher based in Ohio. He is the developer of the Beach Safety Hierarchy Assessment Scale and the author of Lead with Safety.
The Beach Safety Hierarchy was developed through direct observation within an intimate relationship affected by Dissociative Identity Disorder and subsequently grounded in the primary clinical and neuroscientific literature, including the work of Porges (polyvagal theory), Bowlby and Fonagy (attachment and mentalization), Ogden and Fisher (sensorimotor psychotherapy), van der Kolk (traumatic stress), Siegel (window of tolerance), and van der Hart, Nijenhuis, and Steele (structural dissociation). The model was evaluated through administration of the BSHAS instrument to N = 320 respondents across 160 paired dyads.
Scott has presented at the University of Findlay, University of Bluffton, University of Toledo, and Ohio Northern University, and has testified before the Ohio Joint Committee on Agency Rule Review (JCARR) on chemical dependency policy. He currently serves on the board of Focus Recovery and Wellness Community and coordinates the Quick Response Team for post-overdose engagement in Hancock County, Ohio.
Correspondence: scottbeach137@gmail.com